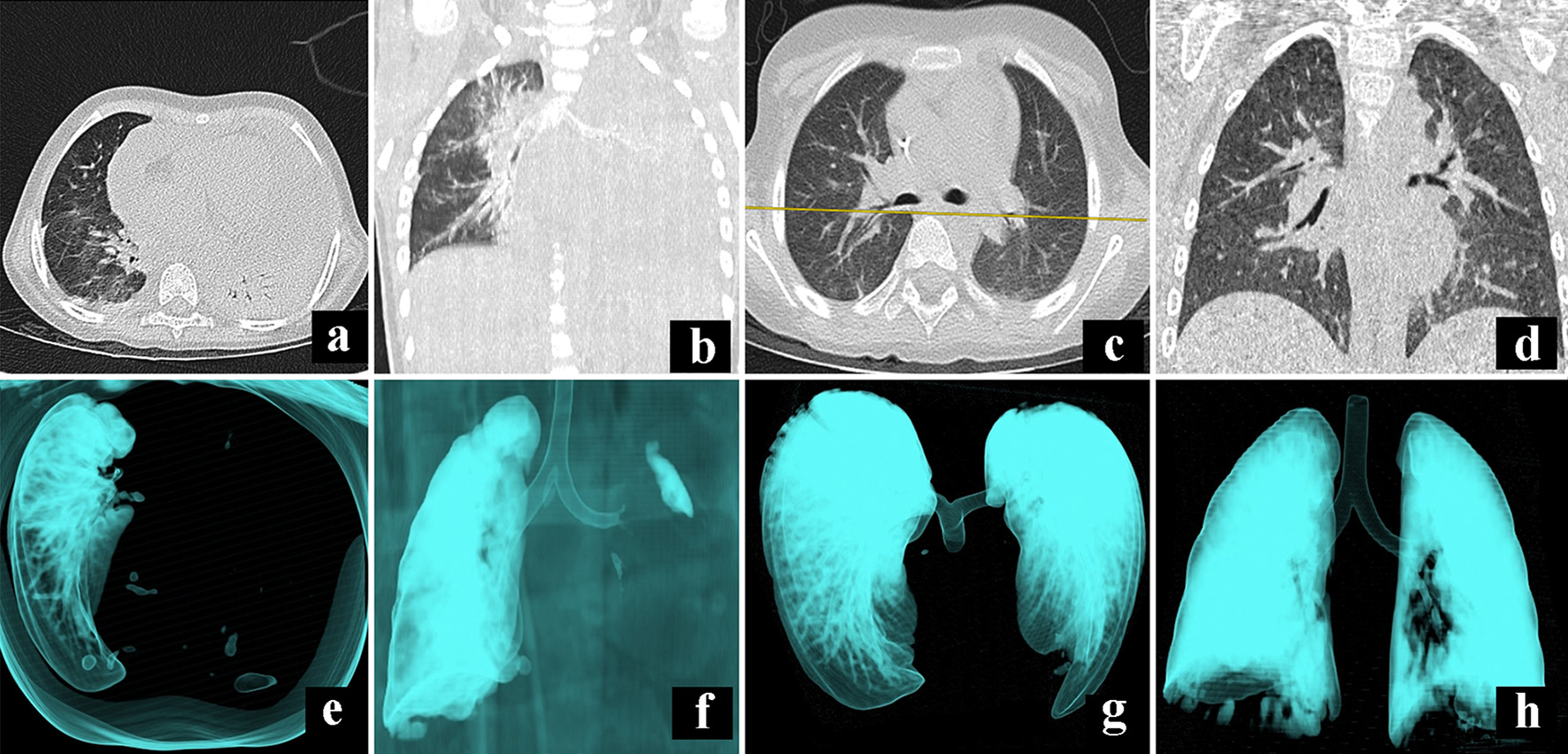
Figure 1. Comparative illustration of CT scan during admission (a, b, e, f) and first discharge (c, d, g, h). Panels (a) and (b) show a massive pleural effusion of the left lung that compromises all the segments; panels (e) and (f) show a 3D reconstruction to denote the occlusion of the left airway. Panels (c) and (d) show the absence of fluid in the pleural space after 18 days of treatment, while panels (g) and (h) show a full expansion of the lungs. CT: computed tomography.
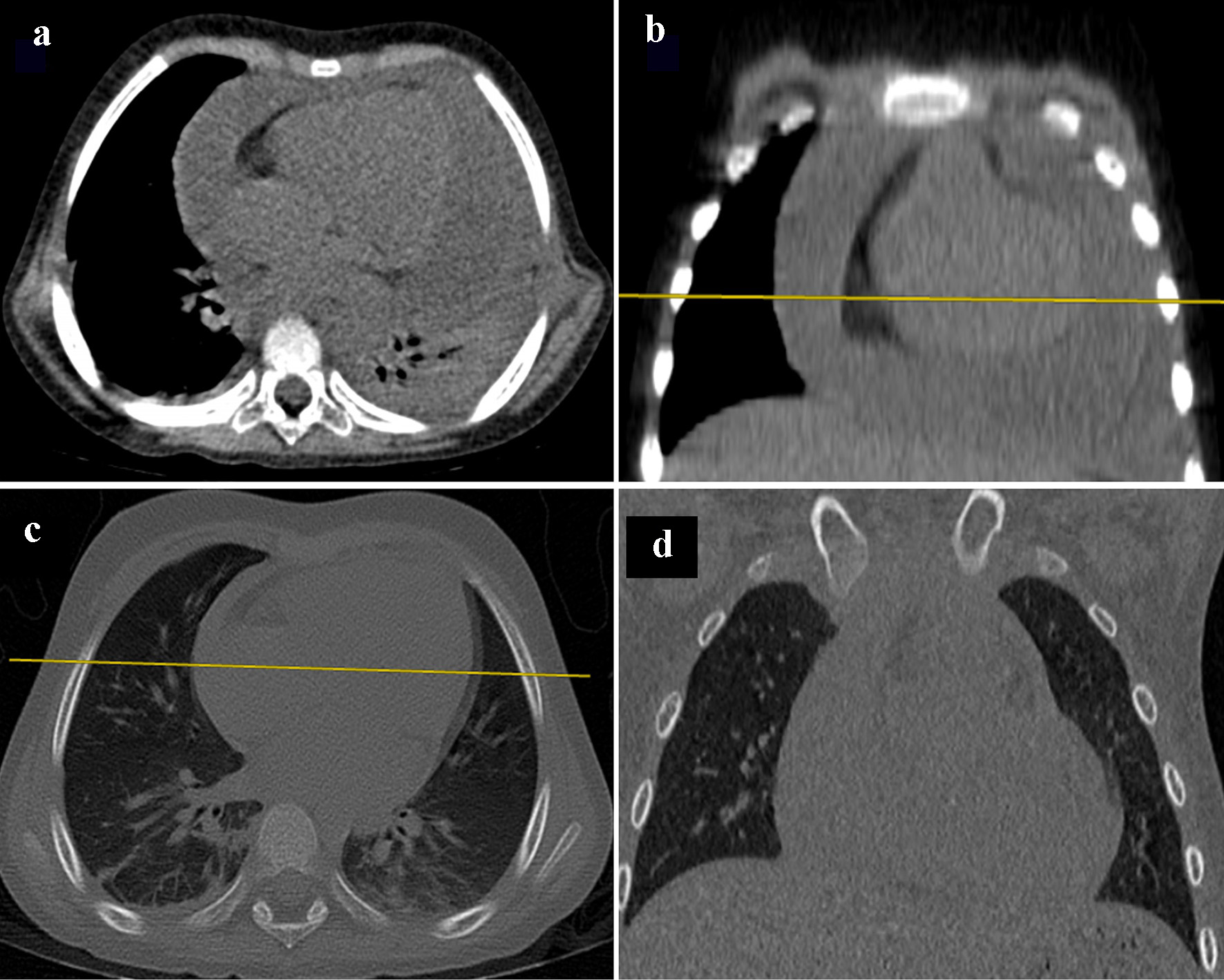
Figure 2. Pleural effusion image. In panels (a) and (b), CT scan of the mediastinum, with axial and coronal planes, show an increase of fluid in pericardial space. However, after treatment with diuretic therapy, comparative panels (c) and (d), the fluid collected in pleural space has diminished. CT: computed tomography.
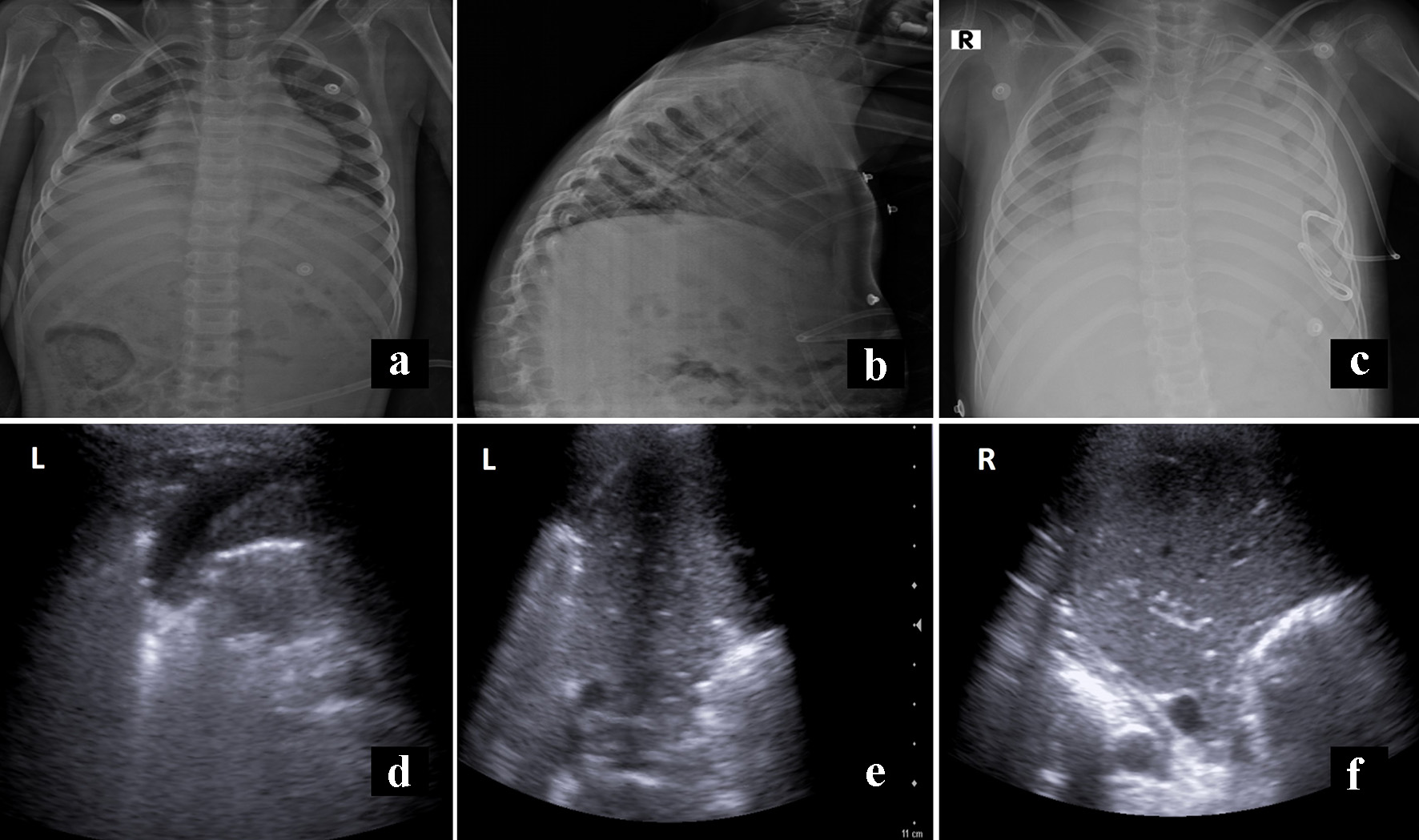
Figure 3. Panels (a) and (b) show the X-ray film before the first discharge without evidence of effusion. Panel (c) shows the initial film to second hospital readmission, with recurrent pleural effusion. Panels (d) and (e) correspond to sonography, previous to definitive discharge, with minimal fluid on the left side (L). In contrast, panel f shows lung parenchyma without fluid (R).